Baby Tibin K, Sunil S, Thomas Eapen, Vijay Naveen
1 Departrment of Oral & Maxillofacial Pathology, Pushpagiri College of Dental Science, Tiruvalla, Kerala
2Department of Oral & Maxillofacial Surgery, Pushpagiri College of Dental Science, Tiruvalla, Kerala
Running title – Central Ossifying fibroma of Maxilla
Received: 11-06-2023
Revised: 15-06-2023
Accepted: 22-06-2023
Address for correspondence: Dr.Tibin K Baby, Reader, Departrment of Oral Pathology, Pushpagiri college of Dental Science, Tiruvalla, Kerala
Email:tibinkbaby@gmail.com
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-Noncommercial ShareAlike 4.0 license, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms
How to cite this article: Baby T K, Sunil S, Thomas E, Vijay N. Massive Central Ossifying Fibroma of Maxilla Involving Maxillary Sinus – An Unusual Presentation. J Oral Biomed Sci 2023; 2(2):87-91
Abstract
Central ossifying fibroma is a rare benign fibro-osseous neoplasm which has a predilection for mandible. It originates from the mesenchymal blast cells of the periodontal ligament and has the capacity to produce bone, cementum, and fibrous tissue. It is a well-defined lesion primarily made of fibrous tissue, with small bits of bone, cementum, or tissue that looks like osteocementum. It is commonly seen in young adults with a female predilection. Herewith, we report a rare case of central ossifying fibroma affecting the right maxilla involving the maxillary sinus in a 73-year-old male patient.
Keywords: Central ossifying fibroma, maxillary sinus, fibro osseous lesions, cementifying fibroma
INTRODUCTION
Central cemento ossifying fibromas, also known as central ossifying fibromas (COF) or central cementifying fibromas are unusual benign fibroosseous lesions of the maxilla and mandible which are thought to originate from the periodontal ligament.1
Ossifying fibromas frequently develop in middle-aged people, primarily in the posterior region of the mandible. They tend to have a female predilection and can also very rarely develop in the maxillary region, paranasal sinuses, or the orbit.2 The first ever case of an ossifying fibroma was reported in 1872 by Menzel and Montgomery coined the term “ossifying fibroma” in 1927.3,4
COF are generally small and can be diagnosed with routine dental radiographs. Cone Beam Computed-Tomography scan is preferred, as it can diagnose and understand the invasiveness of the lesion.5 Patients may complain of an abnormal bite or an enlarging mass, when the lesion is large.1 We present our experience with an unusual aggressive COF of the maxilla involving the maxillary sinus in 73 year old male patient.
CASE PRESENTATION
A 73-year-old male patient presented with pain and swelling in the right upper jaw for past two weeks. On history taking, he revealed that swelling was noted from previous six months. Medical history of the patient revealed an intake of anti- epileptic medication for the past 40 years. Extra oral examination could reveal a notable facial asymmetry with mild non-tender swelling in the right maxilla. Nasolabial obliteration was also noticed on the right side. Patient also had paresthesia over right lateral aspect of the nose.
Enlargement of the right maxilla, spanning from the upper incisor region to the maxillary tuberosity region, was observed during intraoral examination. (Figure-1) On the buccal and palatal sides of the lesion, the mucosa exhibited erythematous alterations. All maxillary anterior teeth and premolars were missing except 15 (root stump).
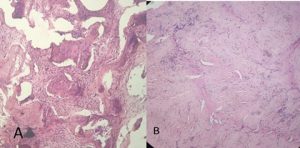
Both coronal and axial sections of the Cone-Beam Computed Tomography scan revealed a mixed radiopaque and radiolucent lesion, involving the right front maxilla, invading to the right maxillary sinus. The right maxillary sinus was obliterated almost two-thirds of its size, with an ill-defined border.(Figure-2) Co-relating case history, clinical features and radiological features, the case was provisionally diagnosed as a fibro osseous lesion. An incisional biopsy was performed, which revealed a hyper cellular fibrous connective tissue stroma with osseous and cementum like materials inclusions. (Figure-3) So the case was diagnosed as ossifying fibroma and patient was advised for partial maxillectomy under general anesthesia.
DISCUSSION
The World Health Organization (WHO) in 1971 categorized four types of cementum containing lesions. They included: fibrous dysplasia, ossifying fibroma, cementifying fibroma and COF.6 In a subsequent WHO classification, osteogenic neoplasms and non-neoplastic bone lesions were separated into two groups to describe benign fibro-osseous lesions in the oral and maxillofacial regions. Cementifying ossifying fibroma was classified under osteogenic neoplasms. However, in 2005, WHO reduced the term ‘‘cementifying ossifying fibroma’’ to “ossifying fibroma”.7,8
The benign fibro-osseous lesion, COF, can develop in the bones of the head and neck. It is regarded as a rare, regionally aggressive, and steadily expanding tumour. The maxilla, as observed in this case, and the paranasal sinus are rarely affected, while the mandible accounts for more than 70% of cases.9-13 They develop as a result of two processes: the excessive proliferation of periodontal ligament cells, and the emergence of a metaplastic process in connective tissue fibres with nonperiodontal origins. These two factors, with the former being more prevalent, could be responsible for ossifying fibroma.14 COF of the jaws has been linked to a considerable increase in mesenchymal cellular induction into bone and cementum, which is necessary for odontogenesis. The lesion in the jaws may arise due to a flaw in the tissue induction method, trauma, periodontitis or previous extractions. 15
The clinical signs of COF can range from mild to aggressive behaviour. Usually, the condition is asymptomatic at the time of discovery.16 The development of COF can produce a noticeable swelling and mild deformity including displacement of teeth.17 Other observed symptoms include nasal obstruction, headache, proptosis and ocular symptoms, such as visual loss and diplopia.9,11,18 COF are typically solitary and well defined lesions. In our case, since the tumour was advancing into the maxillary sinus, there was only a mild external swelling noticed, which may have been the reason for the late diagnosis. In another case report of COF in maxilla in a younger patient, the clinical presentation was difficulty in mastication.5
COF can be distinguished from other fibro-osseous disorders of the jaw using radiography.19 It initially presents as a radiolucent lesion without any evidence of internal radiopacities. The radiolucent area becomes flecked with opacities as the tumour progresses, and eventually the lesion takes on the appearance of a highly radiopaque mass.17 The presented case showed a mixed radiolucent and radiopaque lesion. The general growth pattern of the COF is centrifugal, resulting in cortical proliferation parallel to the growth area and enlargement in all directions.20 The growing pattern in our case was not centrifugal, it could be due to the invasion into the maxillary sinus, the least resistant route. So the clinical swelling was much less than the radiological findings.
Histopathologically, ossifying fibroma constitutes fibrous tissue that contain varying degrees of mineralized material and cellularity. This case showed a hypercellular stroma with osseous and cementum like materials in the connective tissue. Contrary to fibrous dysplasia, the bone may exhibit osteoblastic rimming and spherical calcified deposits that are very acellular and resemble cementum.20
The highly cellular structure of the stroma in these lesions, which demands complete surgical excision to prevent local recurrence, reflects the aggressiveness of the lesion. For minor tumours, this can be accomplished by conservative surgical excision, and for larger lesions, aggressive resection is required. The reported rates of recurrence, which range from 14 to 38%, may be due to variances in the follow-up length or the partial removal.14,21,22
CONCLUSION
Ossifying fibroma is an uncommon benign tumour. As the tumour is clinically asymptomatic, it is first noticed by investigations related to esthetic and dental issues. CBCT is crucial for identifying the lesion’s aggressiveness and the extent to which it has affected nearby structures. As COF is a well-circumscribed lesion, most cases are treated by a conservative surgical excision to preserve esthetics and function. When the lesion is aggressive, and invades into adjacent structures, a radical resection is preferred. Care should be taken to remove the tumour completely and not leave any remnants to prevent recurrences.
Conflict of interest: None
Source of support: Nil
REFERENCES
- John Kuta AJ, Worley CM, Kaugars GE. Central cementoossifying fibroma of the maxillary sinus: a review of six cases. AJNR Am J Neuroradiol. 1995 ;16:1282-6.
- MacDonald-Jankowski DS: Ossifying fibroma: a systematic review . Dentomaxillofac Radiol. 2009, 38:495- 513.
- J.C. Martins Junior, F.S. Keim, M.S. Kreibich, Peripheral ossifying fibroma of the maxilla: case report, Int. Arch. Otorhino-laryngol.2008;12; 295–299.
- I. Baumann, R. Zimmermann, F. Dammann, M.M. Maassen, Ossifying fibroma of the ethmoid involving the orbit and the skull base, Otolaryngol. Head Neck Surg. 2005;133 ;1; 158–159
- Bhat SV, Kumar SP, Periasamy S, Krishna VK, KRISHNA VK. An uncommon presentation of ossifying fibroma in the maxilla. Cureus. 2022; 30;14;3.
- Pindborg JJ, Kramer IRH. Histological typing of odontogenic tumors, jaw cysts and allied lesions. In: International histological classification of tumors. Geneva: WHO; 1971:31‒34.
- Kramer IRH, Pindborg JJ, Shear M. Neoplasm and other lesions related to bone. Histologic typing of odontogenic tumors. World Health Organization. New York: Springer-Verlag; 1992:28‒31.
- Reichart PA, Philipsen HP, Scuibba JJ. The new classification of head and neck Tumors (WHO)- any changes? Oral Oncol. 2006;428:757‒758.
- Zhaleh Mohsenifar, Saeedallah Nouhi, Fatemeh Mashhadi Abbas, Sareh Farhadi, Behzad Abedin, Ossifying fibroma of the ethmoid sinus: report of a rare case and review of literature, J. Res. Med. Sci. 2011;16;6 ;841–847.
- Y.C. Choi, E.J. Jeon, Y.S. Park, Ossifying fibroma arising in the right ethmoid sinus and nasal cavity, Int. J. Pediatr. Otorhinolaryngol. 2000;54 ;2–3;159–162.
- R.P. Manes, M.W. Ryan, P.S. Batra, et al., Ossifying fibroma of the nose and paranasal sinuses, Int. Forum Allergy Rhinol.2013; 3 ;161–168.
- Anirban Chatterjee, Neha Ajmera, Amit Singh, Peripheral cemento-ossifying fibroma of maxilla, J. Indian Soc. Periodontol.2010; 14 ; 3; 186–189.
- S.Y. Lam, N.M. Ramli, D. Harikrishnan, S.F. Sia, J. Pailoor, Ossifying fibroma of the occipital bone—a case report and literature review, Eur. J. Radiol. Extra 2008 ;67 ;1 ;19–23.
- Liu Y, Wang H, You M, Yang Z, Miao J, Shimizutani K, Koseki T: Ossifying fibromas of the jaw bone: 20 cases. Dentomaxillofac Radiol. 2010, 39:57-63.
- Urs AB, Kumar P, Arora S, Augustine J: Clinicopathologic and radiologic correlation of ossifying fibroma and juvenile ossifying fibroma: an institutional study of 22 cases. Ann Diagn Pathol. 2013, 17:198-203.
- White ST, Pharoah MI. Oral radiology principles and interpretation. 6th ed. Missouri: Mosby Elsevier; 2009.
- Sarwar HG, Jindal MK, Ahmad SS. Cementoossifying fibroma: A rare case. J Indian Soc Pedod Prev Dent 2008;26:12831.
- Shekhar Charavarty, Debashish Datta, Esha Boro, Bijita Dutta, Ossifying fibroma in the sinonasal tract: a rare case report, J. Clin. Diagn. Res.2014;8 FD09–FD10.
- Jih MK, Kim JS: Three types of ossifying fibroma: a report of 4 cases with an analysis of CBCT features . Imaging Sci Dent. 2020, 50:65-71.
- Ono A, Tsukamoto G, Nagatsuka H, et al.: An immunohistochemical evaluation of BMP-2, -4, osteopontin, osteocalcin and PCNA between ossifying fibromas of the jaws and peripheral cemento-ossifying fibromas on the gingiva. Oral Oncol. 2007, 43:339-44.
- Triantafillidou K, Ventis G, Karakinaris G, et al. Ossifying fibroma of the jaws: a clinical study of 14 cases and review of literature. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012;114:193‒199.
- Gunaseelan R, Anantnarayanan P, Ravindramohan E, et al. Large cement-ossifying fibroma of the maxilla causing proptosis: a case report. Oral Surgery, Oral Pathology, Oral Radiology and Endodontology. 2007;104:e21‒e25.
Figure-1 (Original). Clinical photograph showing mild swelling and erythematous changes on right maxilla.

Figure-2. A,B,C,D (Original): CBCT images showing mixed radiopaque and radiolucent lesion in the right maxilla and maxillary sinus.
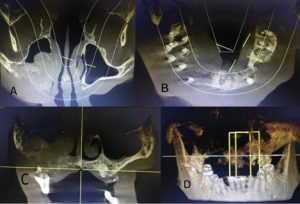
Figure-3 (Original). A: Photomicrograph showing hypercellular fibrous stroma with osseous and cementum like materials (10X) B: Interlacing collagen fibres interspersed by active proliferating fibroblasts. (4X)